






Authored by Dr. Sarika Arora, MD
Ozempic and Wegovy are the leading brand names among a class of weight loss drugs known as GLP-1 receptor agonists (GLP-1 RA’s). They are marketed as breakthrough solutions for weight loss and a host of other health problems.
WHN wants you to know the facts in deciding whether these GLP-1 weight loss drugs are a good choice for you or your family. It’s a fateful decision you have to make in an atmosphere of hype.
Don’t get us wrong – we think these drugs can be great for some women. But over and over, we talk to women who don’t know four basic vital facts about this class of drugs. We want to bring a dose of realism to your thinking about GLP-1 weight loss drugs. This is not to bash them, but to keep from putting them on an impossible pedestal that is bound to disappoint.
So here are the four facts we think every woman should know about Ozempic and its cousins:
Fact #1: Less than half of women find great success with GLP-1 RAs.
Licensing trials for Semaglutide (the active ingredient in Ozempic) showed better results than later “real-world” trials. (This is quite common in the drug-development and launch process.) In the drugmaker-sponsored early trials, over 50% of participants lost more than 15% of their body weight. Later “real-world” trials showed only about half of them achieved such remarkable results. In other study groups, only 25-50% of participants lost more than 10% of their body weight.
The evidence is still early. And for understandable reasons, the drug industry isn’t keen to fund studies that show disappointing results. You should expect that your odds of losing a lot of weight (we are somewhat arbitrarily defining that as 10% or more of your body weight) are no better than 50/50.
Here’s the numbers
Here’s why we chose 10% as a benchmark. For a woman who weighs 200 lbs, a 10% weight loss is 20 lbs. That’s good, but not transformative. The average American woman aged 40 to 49 years old needs to lose ~30 lbs to reach a “normal” healthy weight. But to her, that 10% weight loss (i.e. ~20 lbs) is likely a better result than she ever got from any crash diet.
Studies indicate the average 40- to 49-year-old woman needs to lose ~30 lbs to reach a BMI of 25, the upper limit of what is considered a healthy weight range. This calculation is based on the current average weight for American women in this age range of 178 lbs, which corresponds to a BMI of ~30. That means that the average woman in this age range is right on the dividing line between “overweight” and “obese.” Given an average height of 5’4,” this “average woman” should weigh 146-1/2 lbs to achieve a BMI of 25, implying a weight loss of ~30 lbs, or ~17% of her beginning weight.)
Fact #2: Only about a third of women are still on their GLP-1 RA drug after 1 year.
There are several reasons for women dropping GLP-1 weight loss drugs, and they often overlap:
Side effects.
This is the leading reason women drop Ozempic and its kin. The major adverse side effects are gastrointestinal: nausea, vomiting, diarrhea, constipation and acid reflux. These issues may lessen over time, but are severe enough that many doctors prescribe other drugs during the initial dose escalation phase to mitigate your suffering. But the other drugs bring their own side effects. And for a significant number of women, the side effects are intolerable or not worth it given their disappointing weight loss results.
Disappointing results.
Early results indicate about 10-25% of users experience minimal weight loss or even slight weight gain. These so-called “non-responders” may show little weight loss or quickly reach a plateau at which they stall. There are many theories about why some people fall into this category:
- Those with lower starting BMIs lose less weight.
- Those with better blood sugar metabolism lose less weight.
- Those with certain co-morbid conditions, or on certain drugs, seem more likely to be non-responders.
- Those with prediabetes or metabolic syndrome may respond better. Ironically, those with diagnosed Type 2 diabetes appear to do worse.
High cost.
By now we all know that Ozempic and its kin are expensive. And they’re quite often not covered by your health insurance. Very few women can afford such high out-of-pocket spending, especially since the benefit stops – and the pounds come back on – as soon as you stop. This means that to keep the weight off you have to stay on the drugs for life. Coverage varies by state and insurance plan. We have also heard of women who lost weight only to have their insurance company discontinue coverage. In the company’s view, the health problem was solved. But from the woman’s point of view, she gained back the weight.
Fact #3: There are natural ways to support your own GLP-1 that may be alternatives to weight loss drugs or make it more effective.
Your body makes its own GLP-1, a hormone that is crucial to its regulation of appetite, digestion, glucose utilization, fat storage and related metabolic processes. The “problem” with your natural GLP-1 is that it’s suppressed by a surprising number of factors common to our modern life. Most or all of these are common in women who are overweight:
- Ultra-processed foods
- Low fiber intake
- Low protein diets
- Imbalanced gut flora
- Lack of short-chain fatty acids
- Chronic inflammation
- Poor quality sleep
- Chronic stress or high cortisol
- Obesity
- Insulin resistance/prediabetes
- Poor vagal nerve function
- Aging
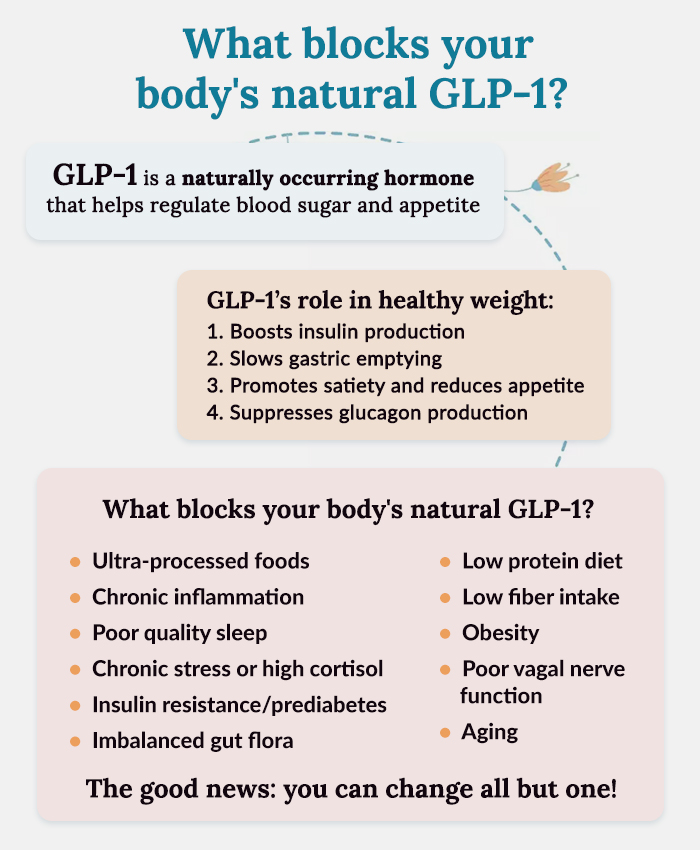
The critical point here is that all but one of those factors are largely or totally within our control. (Aging is the exception!)
Fact #4: You regain any pounds lost after stopping GLP-1 weight loss drugs because they don’t fix the underlying reasons you gained the weight in the first place.
Your body doesn’t put on extra pounds just because you eat too many calories, or the wrong kinds of calories, or too much saturated fat, or any of the dozens of other weight loss theories behind crash diets. All those theories have come and gone – discredited in practice and by science. In fact, cutting edge scientists have known for years that weight gain is a sign of disruption in the body’s very complex system of self-regulation. There is a holistic interplay between hormones, neurotransmitters, gut bacteria, immune function, breathing, diet, exercise and more. This dysregulation creates an equilibrium – what medical science calls a homeostasis – that the body defends, even if it isn’t good for you (often called “weight loss resistance”). You can see this complex mechanism in the factors above that suppress or impair your body’s natural GLP-1.
In one important sense, Ozempic and its cousins prove this model of weight gain. This is because they skip over most of the complex processes that are so hard to fix and zero in on one bottleneck near the end, washing away the subtle signaling with a synthetic drug. But when that drug is removed – as happens with most women, since fewer than a third are still on their GLP-1 drug a year after starting – the weight piles back on. The drug never fixed the dysregulated systems. In fact, it suppressed the body’s own GLP-1 production from its already-low levels, so when you stop it – the inevitable happens.
Finding a real, natural solution
But let’s reframe this: what looks like a problem can be seen as a solution. If we could support the body’s own GLP-1 production while on the GLP-1 drugs, reduce the factors that disrupt the body’s self-regulatory mechanisms and get our internal processes back on track we should be able to lose weight on the drugs and then keep it off. The result would be a healthy weight, all the related benefits and no side effects.
If that’s true, then every woman who is on Ozempic should at the same time pursue a program that supports production of her body’s natural GLP-1.
And for many women who are anxious about taking such a powerful drug – and those who can’t afford to pay for it out-of-pocket – the question is whether she can support her own GLP-1 as an alternative to Ozempic and its kin.



